| |
| Prostatitis (Prostate Infection) |
| |
| What is prostatitis? |
|
|
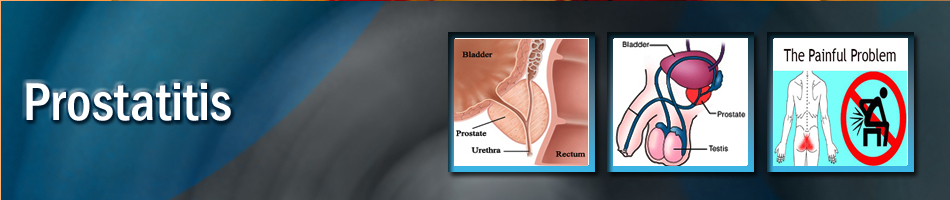
Prostatitis is a condition that involves inflammation of the prostate and sometimes the area around it. There are several types of prostatitis, each with a range of symptoms. Some men with the disease will experience severe pain and others will not be bothered; and the rest fall in between the two. However, the symptoms of the disease do have a significant impact on a man’s quality of life.
|
| |
|
What are the different types of prostatitis and their causes? |
|
|
Acute bacterial prostatitis is the least common type of prostatitis but the most easily recognized. It is usually caused by a sudden bacterial infection and easy to diagnose because of the typical symptoms and signs. It is a severe urinary tract infection associated often with fevers and chills, and a visit to a doctor or hospital is required. Acute bacterial prostatitis can affect any age group. The symptoms include painful urination; inability to empty the bladder, pain in the lower back, abdomen or pelvic area; and fever and chills.
Chronic bacterial prostatitis is similar to acute bacterial prostatitis but the symptoms develop gradually and are less severe. Characterized by recurrent urinary tract infections in men; this condition can affect any age group but is most common in young and middle-aged men.
Chronic prostatitis/chronic pelvic pain syndrome/Nonbacterial prostatitis /prostatodynia, is the most common types of prostatitis. The exact cause of this non-bacterial prostatitis condition is unknown. However, the disease could stem from persistent infection, inflammation and/or pelvic muscle spasms. Inflammation in the prostate can also occur without symptoms. For patients experiencing symptoms they do include; pain in the genitals and pelvic area, difficulty or pain urinating, and sometimes pain during or after ejaculation.
Asymptomatic inflammatory prostatitis is prostatitis without symptoms, despite an inflammation of the prostate. Diagnosis is made when the patient is being evaluated for symptoms unrelated to prostatitis. In cases such as these is, evidence of inflammation is found in biopsied tissue or specimens of urine, semen or prostatic fluid. |
| |
|
| What causes prostatitis? |
|
|
The direct causes of prostatitis are not fully known by the medical community. However, there are several accepted theories. Some cases of prostatitis are clearly related to acute and chronic bacterial prostatitis infections. These infections get into the prostate from the urethra by backward flow of infected urine into the prostate ducts. Bacterial prostatitis is not contagious and is not a sexually transmitted disease. A sexual partner cannot catch this infection.
Certain conditions or medical procedures increase the risk of contracting bacterial prostatitis. There is a higher risk if the man has recently had a catheter or other instrument inserted into his urethra, an abnormality of his urinary tract or a recent bladder infection.
Chronic prostatitis/chronic pelvic pain syndrome may be caused by atypical organisms such as chlamydia, mycoplasma (which may be transmitted by sexual contact) ureaplasma or may also be due to a chemical or immunologic reaction to an initial injury or previous infection. The nerves and muscles in the pelvis may cause pain in the area, either as a response to the prostate infection or inflammation or as an isolated problem itself.
|
| |
|
| What are the symptoms of prostatitis? |
|
|
The symptoms depend on the type of prostatitis infection the man is suffering from. Often men do not notice any symptoms, while some experience symptoms similar to that of a urinary tract infection. However, other diseases can cause the same or similar symptoms. It is very important to be evaluated by a medical professional to determine if the patient has prostatitis and which type so that it can be properly treated.
With acute bacterial prostatitis, the symptoms are severe and sudden and may cause the patient to seek emergency medical care. Common symptoms also include chills, fever, severe burning during urination and the inability to empty the bladder.
In chronic bacterial prostatitis, the symptoms are similar to the acute bacterial prostatitis infections but it does not produce a fever. Other symptoms are burning during urination; urinary frequency, especially at night; perineal, testicular, bladder and low back pain; and painful ejaculation. The condition can be episodic, with flare-ups and remissions, associated with infection, treatment and subsequent recurrence.
The symptoms of chronic prostatitis/chronic pelvic pain syndrome include difficult and sometimes painful urination, discomfort or pain in the perineum, bladder, testicles and penis as well as difficult and painful ejaculation. In some cases, these symptoms can be indistinguishable from those described above for chronic bacterial prostatitis.
Fill out the AUA Symptom Score and share the results with your health care provider. |
| |
|
| How is prostatitis diagnosed? |
|
|
The correct diagnosis is very important because the treatment is different for the different types of prostatitis syndromes. In addition, it is extremely important to make sure the symptoms are not from other conditions such as urethritis, cystitis, an enlarged prostate or cancer. To help make an accurate diagnosis, several types of examinations are useful.
One of the tools doctors use in diagnosis is the National Institutes of Health Chronic Prostatitis Symptom Index.
The index is a series of questions about prostatitis symptoms and how much they currently are affecting the patient. Filling it out and sharing the results with your physician helps the patient stay active in their medical care. The questions to this index may be asked several times however, it is important to take the test so the results from the tests can be compared to one another. This is important because it helps determine the effectiveness of treatment.
In addition to completing the questionnaire your physician may request a physical exam. To examine the prostate gland, the physician will perform a digital rectal examination (DRE). The DRE is a simple examination in which the doctor inserts a lubricated, gloved finger into the rectum. The prostate is located just in front of the rectum and below the bladder; the DRE allows the doctor to easily press and feel the prostate.
From the DRE, the physician will be able to determine whether the prostate is enlarged or tender. Lumps or firm areas can suggest the presence of prostate cancer. The physician will also assess the degree of pain or discomfort the patient experiences as he presses the muscles and ligaments of the pelvic floor and perineum. If a man has prostatitis, this examination may produce momentary pain or discomfort but it causes neither damage nor significant prolonged pain.
If the physician requires a closer look at the prostate gland or decides that a biopsy is necessary, he may order a transrectal ultrasound, which allows him to visualize the prostate gland. If you are at risk for cancer, your physician will consider ordering a PSA test. During a prostate infection however, the PSA can be falsely elevated.
If your physician suspects that you have prostatitis or one of the other prostate problems, he may refer you to an urologist, a doctor who specializes in diseases of the urinary tract and male reproductive system, to confirm the diagnosis.
The urologist will repeat some of the examinations already performed by the first physician. The urologist will also assess the degree of pain or discomfort the patient experiences as he presses the prostate. The urologist may analyze various urine specimens as well as a specimen of prostatic fluid obtained by massaging the prostate gland during the DRE. When the prostate is massaged a fluid known as the expressed prostatic excretion (EPS) comes out of the penis. Urine specimens and EPS are analyzed for signs of inflammation and infection. These samples may help the urologist determine whether your problem is inflammation or infection and whether the problem is in the urethra, bladder or prostate. Some doctors may check blood and/or semen samples. With all of these, they are looking for the presence of microorganisms, white blood cells or other indications of infection.
Other tests the urologist may consider using include cystoscopy in which a small telescope is passed through the urethra into the bladder permitting examination of the urethra, prostate and bladder. The urologist may also order urine flow studies, which help measure the strength of your urine flow and any obstruction caused by the prostate, urethra or pelvic muscles.
|
| |
|
| How is prostatitis treated? |
|
|
The treatment for prostatitis depends on the type of infection you have been diagnosed with.
With acute bacterial prostatitis, the patient will need to take antibiotics for a minimum of 14 days. Sometimes, a patient is admitted to the hospital and given intravenous antibiotics. A catheter is sometimes required if the patient has difficulty urinating. Almost all acute infections are cured with this treatment. Frequently, the antibiotics will need to be continued for as long as four weeks. If the patient fails to respond to treatment, the doctor will try other antibiotics.
It is important to know that when taking antibiotics, always follow the doctors’ orders carefully. Do not stop taking the drugs ahead of schedule just because the symptoms go away.
If chronic bacterial prostatitis is diagnosed, the patient will require antibiotics for a longer period, usually four to twelve weeks. About 75 percent of all cases of chronic bacterial prostatitis clear up with this treatment. Sometimes the symptoms come back recur and antibiotic therapy needed again. For cases that do not respond to this treatment, long-term, low dose antibiotic therapy is recommended to relieve the symptoms. Other medications (such as those used for nonbacterial prostatitis) or other treatments (e.g., prostate massage therapy) may also be used in difficult cases. In some rare cases, surgery on either the urethra or prostate may be recommended. There must be a specific anatomic problem, such as scar tissue in the urethra, for any surgery aimed at improving prostatitis to be effective.
The patient may not need antibiotics, if they are diagnosed with chronic pelvic pain syndrome. Frequently, physicians have difficulty trying to decide whether a patient has bacterial or nonbacterial prostatitis. This is because of the difficulties in obtaining a specimen and, sometimes, previous antibiotic therapy obscures the diagnosis. An organism that responds to antibiotics, but is difficult to diagnose may also cause chronic pelvic pain syndrome. For these reasons, antibiotics may be prescribed, at least initially, even when a definitive diagnosis of bacterial prostatitis has not been made with the appropriate tests. Your response to the antibiotic therapy will decide whether or not it should be continued. Many patients without a true infection may feel better during antibiotic therapy because many antibiotics have direct anti-inflammatory effects. Depending on your symptoms, you may receive one of a variety of other treatments. Some doctors prescribed alpha-blockers which help relax the muscles around the prostate and the base of the bladder, relieving any spasms or muscle tightness that contribute to pain with urination. Often anti-inflammatory drugs, pain medications, muscle relaxants, plant extracts (quercetin and/or bee pollen) are used. Repetitive prostatic massages (to drain the prostate ducts) are common treatments to release the fluid that is causing pressure in the prostate.
Hot sitz baths or other various heat therapies (including local heat therapy with hot water bottle or heating pad) relieve the discomfort associated with the infection. If sitting does become too uncomfortable patients are advised to use a pillow or an inflatable cushion. Biofeedback and relaxation exercises may also help to alleviate some of the symptoms. You may be advised to discontinue some foods (e.g. spicy) and drinks (e.g. caffeinated, acidic) and avoid circumstances (e.g. bicycle riding) that exacerbate the problem.
|
| |
|
| |
| Frequently asked questions: |
| |
| Is prostatitis related to prostate cancer? |
|
|
No. Prostatitis is not associated with prostate cancer. Although an inflamed prostate can increase the level of PSA in the blood, having prostatitis is not a sign of prostate cancer, nor does it mean an increased risk of developing prostate cancer in the future.
|
| |
|
| Why do physicians have trouble diagnosing prostatitis? |
|
|
The diagnosis of the various types of prostatitis can be very difficult and sometimes quite frustrating for the patient and his physician. The symptoms are variable and there is much overlap in symptoms between the various types of prostatitis. Once the patient has been treated with antibiotics, it can be difficult to differentiate a bacterial prostatitis from chronic pelvic pain syndrome.
|
| |
|
| How will prostatitis affect a patient? |
|
|
It can seriously affect a patient's quality of life. The correct diagnosis of the prostatitis problem is difficult and it is not always cured. However, prostatitis is a treatable disease and one can usually get relief from major symptoms by following the recommended treatment.
|
| |
|
| Did my partner’s urinary tract infection (UTI) cause my prostatitis? |
|
|
Bacterial prostatitis is not contagious. There is still much to learn about non-bacterial prostatitis, and there may be multiple causes for it. Some cases may be due to Chlamydia, an organism that can be sexually transmitted, but prostatitis has never been associated with a partner’s UTI.
|
| |
|
| Why are some patients not cured after they have been diagnosed with prostatitis? |
|
|
Most cases of acute bacterial prostatitis respond completely to therapy. Unfortunately, the treatment for the chronic prostatitis syndrome is far from perfect. Patients with chronic bacterial prostatitis can have persistence of their infectious problem despite antibiotic use. This is because of the difficulty antibiotics have in penetrating the prostate gland to completely kill all the bacteria deep within the prostatic ducts. Repetitive or frequent prostate massages or use of alpha blockers may be helpful in these cases. The patients who have had chronic bacterial prostatitis and have been cured are susceptible to recurrences. Many patients with chronic prostatitis/chronic pelvic pain syndrome fail therapy. The physician may employ a multi-modal approach to therapy (more than one treatment at a time). Patients may find that they have to learn to live, and cope with their symptoms while the inflammation hopefully "burns itself out."
What are some of the most important facts about prostatitis?
» Correct diagnosis is the key to the management of prostatitis.
» Prostatitis cannot always be cured but can be managed.
» Treatment should be followed even if symptoms have improved.
» Patients with prostatitis are not at higher risk for developing prostate cancer.
» There is no reason to discontinue normal sexual relations unless they are uncomfortable, usually during an acute phase.
»One can live a reasonably normal life with prostatitis |
| |
|
| |
| |
|
| |
|
|
 |
Endoscopic removal of urinary stones: PCNL, URS, RIRS, CLT |
|
|
LITHOTRIPSY (ESWL) |
|
|
LASERS for stones and Prostate |
|
|
Monopolar and bipolar TURP |
|
|
HOLEP |
|
|
Urodynamics and uroflowmetry |
|
|
Laparoscopic urology surgeries |
|
|
Paediatric urology surgeries |
|
|
Urinary incontinence surgeries |
|
|
Surgeries for genitourinary cancers |
|
|
Reconstructive urology |
|
|
Microsurgeries for infertility and impotence |
|
| |
|
| |
 |
|